

Editor’s Note: The following post is taken from the Q&A session of IntegriChain’s ‘How to Self Police Revenue Leakage due to 340B Program Non-Compliance’ webinar. Dave Weiss, Executive Director, Industry Solutions, lead the presentation. Dave’s responses have been edited for clarity. Click here to view the full webinar recording.
Q: Can you address the eligibility of orphan drugs for 340B pricing at 340B sites that were added as part of the Affordable Care Act (ACA)? It is my understanding that an orphan drug used “on label” is not eligible for 340B pricing in these expanded sites [newly eligible covered entities]. Can you confirm?
A: Yes, that is our understanding of the regulation as it is written. Covered entities newly eligible as part of the Affordable Care Act (ACA) are not eligible to receive 340B pricing for orphan drugs used “on label.”
The Orphan Drugs Exclusion summary on the HRSA website states, “The interpretive rule outlines the agency’s interpretation that the 340B statute requires manufacturers to offer entities newly eligible for 340B under the Affordable Care Act 340B pricing on drugs that have received an orphan designation when those drugs are used for their non-orphan indication.”
Q: Has there been similar growth in contract pharmacy child sites versus the ~4,500 parent sites to date?
A: The rapid growth in contract pharmacy sites we presented during the webinar were child sites, not parent sites. The number of contract pharmacies exploded by 280% from 2015-2018. Growth could be even more staggering as Figure 1 below accounts for only the first 6 months of 2018.
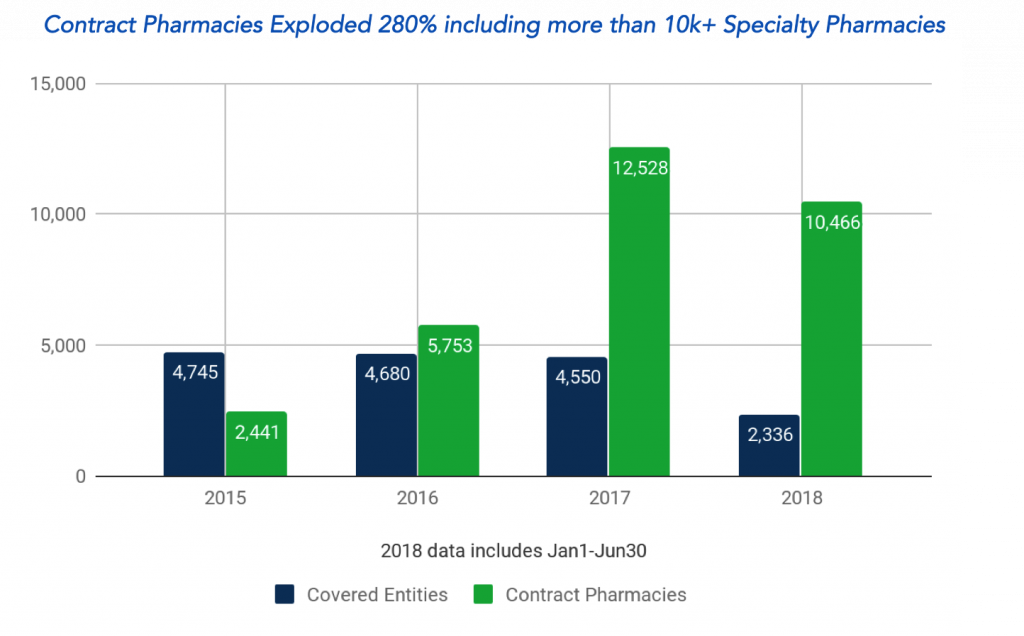
Figure 1: 340B covered entity and contract pharmacy trends 2015-18. Source – IntegriChain analysis of HRSA Program Integrity Audits 2018
Contact specialty pharmacy growth is accelerating as well. In the Immunology class alone, we observed an overall 150-200% increase in specialty contract pharmacy purchases.
Q: What is diversion?
A: Diversion is the transfer of drugs at 340B prices to ineligible patients. A few examples of how diversion happens are:
- Drug dispensed at a contract pharmacy for a prescription written at an ineligible site
- 340B drugs dispensed to ineligible patients
- Drug dispensed at an entity not supported by medical records
- Drug dispensed at a contract pharmacy with no documented provider/patient relationships
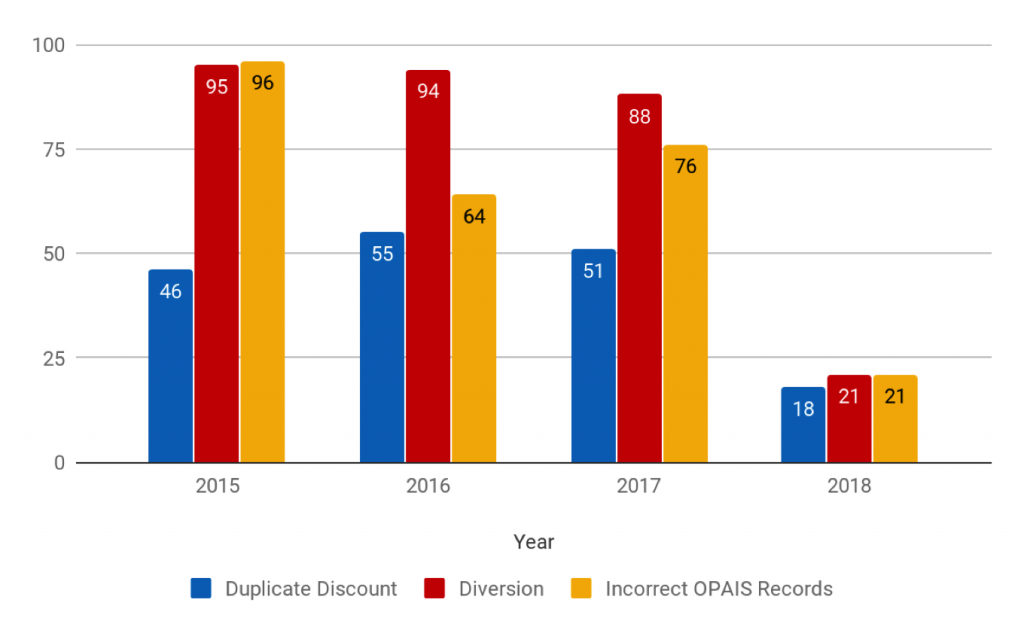
Figure 2: Prevalence of different types of 340B program non-compliance. Source – IntegriChain analysis of HRSA Program Integrity Audits 2014-18
IntegriChain’s analysis shows that diversion is by far the most prevalent adverse finding (Figure 2 above) but most difficult for pharmaceutical manufacturers to address.
Section 602 of the Veterans Healthcare Act of 1992 provides guidelines for determining if an individual is in fact a “patient” of a covered entity:
-
The covered entity has established a relationship with the individual, such that the covered entity maintains records of the individual’s healthcare
-
The individual receives healthcare services from a healthcare professional who is either employed by the covered entity or provides healthcare under contractual or other arrangements (e.g., referral for consultation) such that responsibility for the care provided remains with the covered entity
-
The individual receives a health care service or range of services from the covered entity which is consistent with the service or range of services for which grant funding or Federally-qualified health center look-alike status has been provided to the entity. Disproportionate share hospitals (DSH) are exempt from this requirement.
Q: How can a pharma manufacturer gain visibility to Bill-To and Ship-To hierarchies using IntegriChain’s 340B data solutions?
A: If you’re a current IntegriChain customer and using our datasets, you’re probably familiar with the National dataset. The National dataset is the enriched, unblinded version of 867 data. This dataset includes Ex-factory and returns. IntegriChain National data provides visibility at an entity level, e.g., University of Pennsylvania Health System plus Class of Trade (COT) with that entity. The COT master includes inpatient pharmacies, 340B contract pharmacies, and 340B outpatient pharmacies.
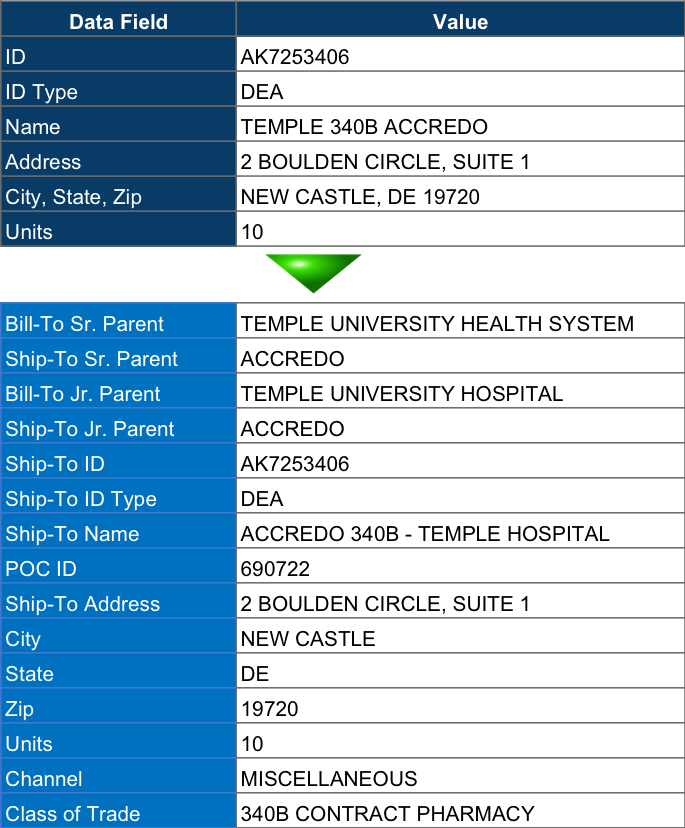
Figure 3: An example of the Bill-To and Ship-To hierarchies available as part of IntegriChain’s 340B solutions
A greater level of detail and 340B program monitoring is available with IntegriChain’s Subnational dataset. Subnational is the enriched, unblinded version of 867 data that includes specific addresses and sites of care. This dataset provides individual pharmacy purchase volume and sales mix details for each 340B and non-340B site of care.
If you’re a customer, but not an IntegriChain 340B Analytics customer, you typically will NOT see the Bill-To hierarchy. You can get to COT level reporting but you won’t necessarily see the Bill-To hierarchy. When you sign on for 340B Analytics, we expose the Bill-To hierarchy as part of that solution.
Existing users should speak to their IntegriChain Account Manager about turning on Bill-To hierarchies. New customers can email sales@integrichain.com for more information on IntegriChain’s 340B solutions.
Q: Is there any validation of a 340B entity other than the PHS or DSH designation in the [covered entity] name?
A: When we’re adjudicating chargeback and rebate transactions, our operations team will validate covered entities and contract pharmacies against the Office of Pharmacy Affairs 340B OPAIS database. The 340B Analytics do not presuppose we’re performing this services. The analytic itself doesn’t validate eligibility against the OPAIS database. We assume that step is done as transactions are processed at their source.
As it relates to IntegriChain 340B Analytics, we assume that the data is coming from a chargeback. And we’re assuming your chargeback system has validated that entity under the contract. If we’re looking at a more direct sale situation or the data is 867, we’re making the assumption that your wholesaler trade partner has done that validation at the source. When we look at 867, we don’t necessarily go back and re-validate against the HRSA database. We assume, in this case, your wholesale distributor has done that. That’s what they’ve agreed to do.
We do perform some validation checks in retrospect, but we don’t validate as the transaction data comes in. We do validate at the location. We validate the units. We validate the class of trade (COT). We’re just looking at that designation (DSH or PHS) which tells us that transaction is encoded as 340B. It’s not what we’re using to assign class of trade.
About the Author

Dave Weiss
David Weiss, a software industry veteran, is charged with leading IntegriChain’s effort to provide pre-sales business consulting to life sciences manufacturers in the areas of needs assessment, analytics design, and value engineering. Prior to IntegriChain, David led the solutions and product marketing organizations at Model N, SAP, and IDS as well as spent five years as a management consultant for PWC, KPMG, and Knowledgent.






